THE concept of Herd Immunity is premised on the following facts:
That a vaccine, given to a majority of a given population at about the same time raises immunity of that population in that community so that the infective organism cannot find susceptible persons to infect easily and hence peters away in that community. In general, if about 80% in the community are vaccinated, the antibody levels will be uniformly similar in all those who are vaccinated so that the remaining 20 % do not get the infection.
Some virologists and epidemiologists want to apply this concept of herd immunity to the present pandemic. Their recommendations are based on following assumptions:
- This is essentially a viral illness with less mortality.
- Only vulnerable with co-morbidities like diabetes get serious complications and some of them may probably die.
- Most remain asymptomatic. Varying figures are given; according to the Government of Tamil Nadu it is over 80% in TN.
- Among those who develop symptoms, most develop mild symptoms like fever or cough which are mostly self-limiting . Less than 1% develops serious complications and they can be treated in ICUs.
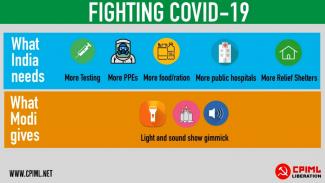
- Lockdowns have not prevented the spread and result in huge economic loss to the country and the poor are the worst affected.
- 6] There are no known specific medicines and a vaccine against this virus, if at all possible, is certainly at least a year away.
- Therefore open up all economic activities. Most people will get asymptomatic viremia and among those who develop symptoms, less than 1% may become seriously ill and some old people with co-morbidities would die. This is something similar to the annual influenza death in the US or UK and nothing more. This way we can get over this pandemic with less human and social loss and at the shortest possible time.
This looks attractive in theory. This is politically popular too because we are talking about preventing poor people dying of hunger and other diseases due to lockdown. Lifting lockdown may end their financial miseries.
But if we look at this disease more carefully we notice:
- This virus is totally unknown to humanity.
- It does not have stereotypical behaviour. The death rate varies widely across countries and even inside countries it varies from region to region. In India it is around 3 to 4 %. In TN it is less than 1%. Globally it is around 6.5%. Almost all countries like to underreport fatalities; hence published fatalities will always be lesser than the actual fatalities, more so in third world countries where data fudging is easy.
- We still do not know if the majority remain asymptomatic. Spain, Italy, UK and US experiences are to the contrary. Most infected people had moderate to severe symptoms and needed hospitalisation and ventilation etc. We have seen how health systems were crippled and thrown out of gear in most European countries and USA.
- It is far too simplistic to say that only old and vulnerable people die. The South American example especially Brazil disproves this assumption quite conclusively. 15% of deaths in Brazil are in the age group under 50. Mexico is worse. One quarter of all deaths in Mexico are in the age group 25 to 49. Many people do not realise that even in India about 50% of deaths are in people below the age of 60.
- This disease is certainly not like flu. Even amongst those who become symptomatic, it runs a variable course. It leaves lasting damage on organs like lungs and kidneys in many patients. Some people suffer for as long as 40 days. So simplistic conclusions about this disease are wrong. In severely ill patients the outcomes are simply unpredictable. More than 90% of those who required ventilators did not come out of it alive in the initial period. Now with better understanding of the peculiar pathology of this disease the ventilator fatality is reduced to around 50%. Those who come out have severe multi-organ injuries and lasting morbidities.
- It induces a pro-thrombotic state and there are serious discussions in professional circles that many sudden heart attacks and strokes may be due to this.
- Many countries are already speaking about the second wave. Even after such a severe spread in Spain, the recent random antibody testing shows that only 5% have detectable high titre of antibodies. In other words, 95% Spaniards are still susceptible to an attack by this virus. If herd immunity cannot develop in Spain, is it realistic to expect that it may do so elsewhere especially in a country like India?
- Except for states like TN and Kerala, the care for those poor people who develop serious infection needing ICU care/ventilation, is virtually non-existent in most states. Private sector is extremely expensive and even that is not available in many states. Therefore it is a dangerous thing to open up without having the ability to manage the consequences.
- According to one calculation, to achieve herd immunity in India, at least 80 to 90 crore people should be infected [about 60 to 70% of the population] of which 8 to 9 crore [10% of the infected persons] would require hospitalisation and about 80 lakhs to 2.7crores [1-3%] will die. Do we have ICU facilities for such numbers and is this mortality socially acceptable?
Therefore to parrot herd immunity theory is not very convincing medically. It is welcome if it happens as a result of widespread infection. But to deliberately expose a huge population with the hope of development of herd immunity is not scientifically convincing. Let me reiterate that for this present pandemic herd immunity is still largely a theoretical construct.
To come to the practical aspects: we have seen that though this virus entered this country through airports, it nestles in the slums of Mumbai, Ahmedabad and Chennai. It is true that lockdown affects the poor more than the rich who have means to survive many months of lockdown without many problems. It is also equally true that once opened, it is the poor who are going to work in sweatshops and shop floors and get infected. The rich will certainly protect themselves well and it is the poor who are going to get more infections when lockdown is lifted. In New York, death rate in low income communities of colour is 10 times greater than the wealthier ones. When we talk about exposing the 80% to protect the 20% we must be very clear as to who form this 80% and who form the 20%. When we talk about protecting the vulnerable, we are really talking about the rich and vulnerable and not the poor and vulnerable. The poor people of India still live in joint families where grandparents and grandchildren live huddled in crowded bastis of less than 500 sq.ft. Unlike the affluent West, there are simply no means to protect the poor and vulnerable old people in India.
What then is the way out? Vaccine and antiviral medicines are many years away. Hence the age old wisdom of “Prevention is better than Cure” is very true of this disease with varied manifestations and unpredictable outcomes. This is much, much cheaper than the costs of ‘Herd Immunity’. Fortunately in TN, Maharashtra and in Gujarat, this disease is rampant only in certain pockets. So ideally we must increase our testing numbers drastically in these areas so that the source of these clusters are found out and isolated. It is stupid to follow ICMR guidelines about not testing asymptomatic persons. In these clusters it is the asymptomatic persons who are seeding infections continually and hence our high numbers from the same areas day after day.
And other than these Red Zones and containment areas we should gradually open up economic activities ensuring that the three cardinal principles of prevention – physical distancing, hand washing and masking - are very strictly enforced in public places and places of work at least till this epidemic is brought under control. This works in several countries and this will work in India too. The Swedish way is simply not replicable in India.
Liberation Archive
- 2001-2010
-
2011-2020
- 2011
- 2012
- 2013
- 2014
- 2015
- 2016
- 2017
- 2018
- 2019
-
2020
- Liberation, JANUARY 2020
- Liberation, FEBRUARY 2020
- Liberation, MARCH 2020
- Liberation, APRIL 2020
-
Liberation, MAY-JUNE 2020
- Stand With the Cyclone Ravaged Areas and People : Donate Generously to Relief Efforts
- The Lockdown Has Unlocked India's Suppressed Social Reality of Migrant Workers
- Modi's Covid19 Stimulus Package: Monumentally Deceptive and Disastrous
- Enslaving India's Workers and Renting Out India To Global Capital Is Not the Way to Self Reliance
- Dealing with the Lockdown: Precious Lessons from the Unique Experience of an Unprecedented Phase
- Remembering Ambedkar amidst the Covid19 Pandemic and Lockdown
- May Day 2020 : International Day of Workers in Times of Global Pandemic
- The 202nd Birth Anniversary of Karl Marx
- Experiences of Relief Work in Bihar: Government Abdicates, People take Initiative
- Lockdown Emboldens Feudal, Communal and Criminal Forces
- The Girl on a Bicycle
- Will the Government Not Give Us Jobs?
- Migrant Workers of Jharkhand Stranded in Maharashtra During Lockdown
- Lockdown Relief Reports from Uttar Pradesh
- The Varanasi Mohalla Kitchen Experience
- CPIML Activities in Kerala during the Lockdown
- Initiatives in Tamil Nadu During Lockdown
- Covid 19 Lockdown Relief Work in Chandigarh
- Thousands of Distressed Workers in Jaipur Come Out on the Streets
- Relief Work During Lockdown in Delhi
- Invisible but Irreplaceable? Migrant Labour BC 2019 and AC 2020
- Karnataka : Notes on Migrant Workers Assistance Campaign
- The Pandemic and Beyond : Free Quality Healthcare is a Fundamental Right
- Epidemic Act 1897 : A Draconian Colonial Hangover
- Kerala Model Delivers in Covid -19 Control
- A Note on Herd Immunity
- Modi Regime's War on Working Class
- Attacks on Students and Public Education
- The Pandemic's India Journey: Short Takes
- Open Letter to British Labour Party Leader: Don't Align the Labour Party with Allies of Modi's Far-Right Regime
- Facilitating the Corporate Plunder of Kashmir Under Cover of Covid19
- Hunger Strike by CPIML Leader BN Singh Incarcerated in Medini Nagar, Jharkhand
- Hari Vasudevan
- Tribute : Comrade Narender Kumar & Comrade Suhail Akhtar
- Liberation, JULY 2020
- Liberation, AUGUST 2020
- Liberation, SEPTEMBER 2020
- Liberation, OCTOBER 2020
- Liberation, NOVEMBER 2020
- Liberation, DECEMBER 2020
- 2021-2030



Charu Bhawan, U-90, Shakarpur, Delhi 110092
Phone: +91-11-42785864 | Fax:+91-11-42785864 | +91 9717274961
E-mail: info@cpiml.org